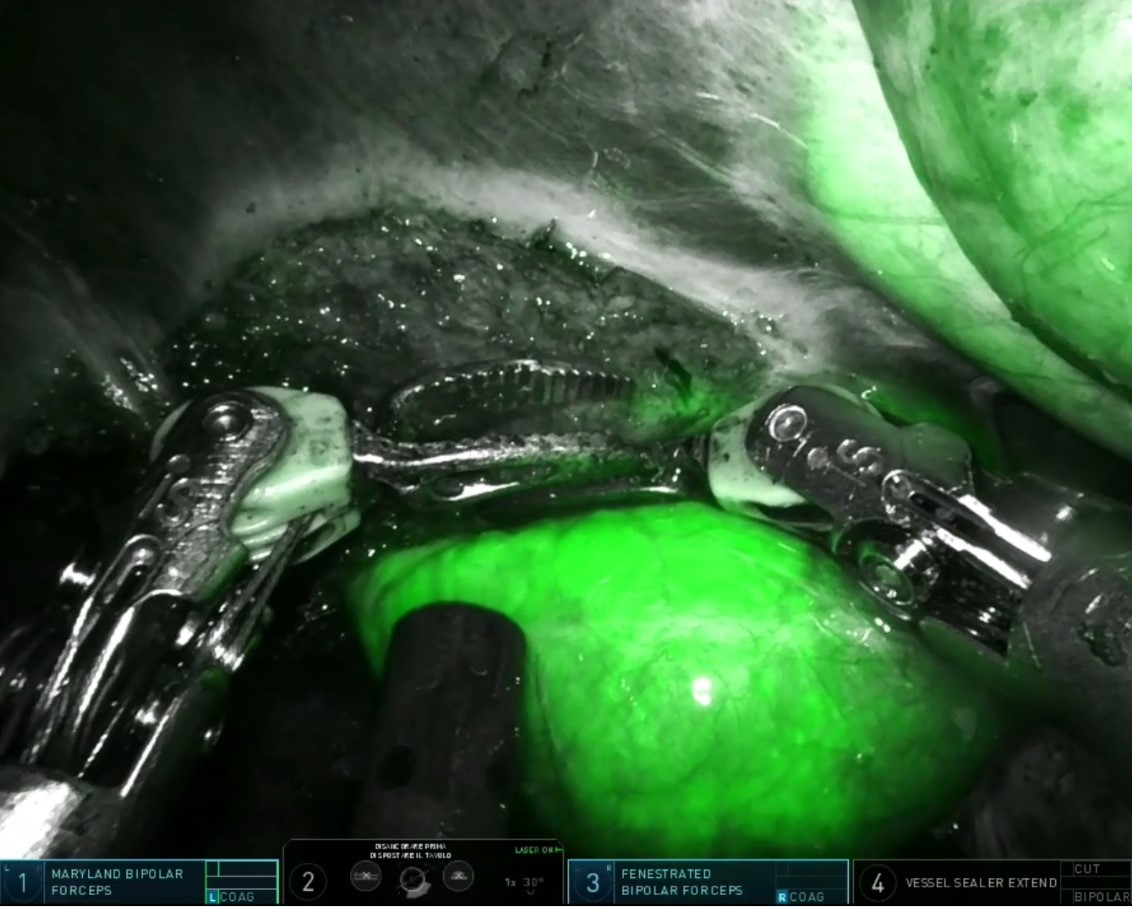
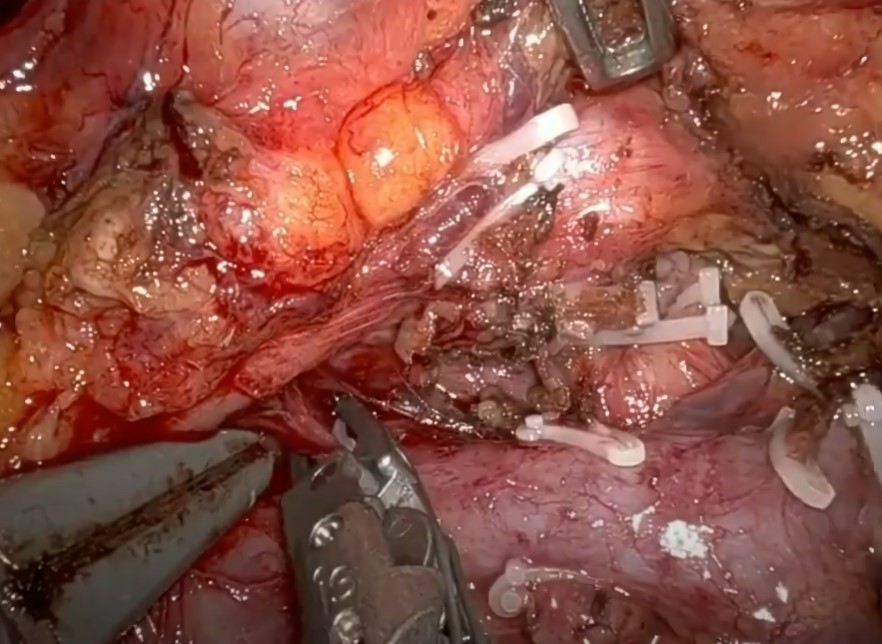
We present the case of a 61-year-old woman followed up for the past 7 years for a dilation of the left biliary tract at the level of the left liver lobe with 3 episodes of angiocholitis. The robot is positioned at the level of the patient’s head. Four ports are put in place. The intervention is begun with placement of the hepatic pedicle on a tape. The liver is then mobilized and the falciform ligament is divided. The hepatotomy is performed at about 1cm to the left of the falciform ligament. The hepatotomy is begun. It is performed by means of the CUSA ultrasonic dissector, and hemostasis and biliostasis are performed using a bipolar grasper. The different elements of the portal pedicle are dissected and controlled. Once the biliary tract has been dissected, it is opened using scissors. As soon as it has been opened, an intrabiliary lithiasis is found. Each stone is progressively extracted to prevent any spillage within the peritoneum. Simple suctions are initiated. A Dormia basket is then placed through the left tract to clear both the convergence and the right biliary tract. Control intraoperative choledochoscopy is performed. New maneuvers are carried out using a series of lavage, allowing for the complete clearance of the biliary tract. Once the voiding of the biliary tract has been controlled, the left biliary tract is closed by means of a PDS 5/0 running suture. The hepatotomy is pursued in order to complete the left lateral sectionectomy. The left supra-hepatic vein is divided by means of an Endo GIA™ linear stapler. The suture and hemostasis are completed by means of different fastened stitches. The tape is removed. The bag containing the stones is extracted by means of a Pfannenstiel’s incision. The postoperative outcome was uneventful and the patient was discharged on postoperative day 6. Final pathological findings ruled out the presence of any malignancy.

Video
Pancreasectomia totale robotica
Pancreasectomia totale robotica per doppia localizzazione di tumore al pancreas